|
|||
1. WHAT IS THE FELDENKRAIS METHOD? |
|||
|
The Feldenkrais Method*(FM) is a process for improving human motor control and awareness. With an emphasis on motor control, the individual learns to move and function better and is freed from chronic stressful habitual movement patterns despite pathology. Pain changes as a consequence of better function. FM utilizes proprioception and motor control for awareness, refinement, control and mastery of movement. Appropriate, accurate and individualized FM can be successfully applied in musculoskeletal medicine as another tool for aiding diagnosis and treatment. Moshe Feldenkrais 1904-1984Feldenkrais earned a Doctor of Science in Physics from the Sorbonne in Paris, where he assisted Nobel Prize winner Joliot-Curie in early nuclear research. Feldenkrais learnt Judo and he became one of the first Europeans to earn a Black Belt in Judo (1936). After suffering knee injuries, he used his own body as his laboratory combined with his knowledge from biology, pediatrics, cybernetics, linguistics, and systems theory. Living and Dead AnatomyGalen and Vesalius dissected human cadavers to define anatomy and function of the human body. This is regional anatomy and function of a dead person. This is a first order classification for human movement. A second order classification of human movement might involve all body segments |
functioning in coordinated action. FM focuses to living regional and global human anatomy. This shift to include regional and global determinations of movement organization and optimization is a major addition to the understanding of human movement in rehabilitation.
This methodology leads to a unique central concept of FM which asserts that because the musculoskeletal system is a system then: “the part that is hurting is moving too much”The region in pain is over stressed in the system and is compensating for another part(s) that is not contributing to movement. A traditional diagnosis stands but interpretations for effective treatment possibilities are increased. The Brain's Sense of Movement and Proprioceptive AcuityMusicians, dancers, chefs and wine tasters all have enhanced learnt abilities with the senses -taste, smell, hearing and also movement and proprioception. To control over 600 muscles and 200 bones the brain needs a sense of the shape and organization of the body and skeleton. Proprioception is the sensory input for the brain's sense of the body's shape, skeletal geometry and movement. The kinaesthetic or sixth sense is defined as our ability to perceive movement. A major premise of FM is that the sixth sense can be enhanced through learning with significant affects upon physical and mental function. |
| * FELDENKRAIS, FELDENKRAIS METHOD and AWARENESS THROUGH MOVEMENT are registered service marks of The FELDENKRAIS GUILD(r). |
| copyright © 1999-2004 robert j burgess. all rights reserved. |
2. THE FELDENKRAIS METHOD - CONDITIONS THAT DO WELL |
|||
Spinal ConditionsAll spinal conditions do well with FM :
Greater awareness and motor control of trunk function provides back pain sufferers with an effective process to better function and out of pain. Chronic conditions
Renewed awareness and learning new movement patterns through FM can be the beginning of a new direction for people with chronic conditions. The use and practice of FM has an accumulative affect unlike many other more palliative treatment processes for chronic conditions. Posture and stressMany people present with a condition that has some relation to posture, stress or the emotions. The gentle learning approach of FM greatly contributes to progress for these “conditions.” Upper limb disordersRestoration of the synergistic relationship between arm and trunk action can aid many upper limb disorders:
|
Sports MedicineThe FM's global biomechanical view of the body can enhance an athlete's performance and aid in addressing the chronic and recurrent problems experienced by sports people. Multiple pain syndromesThe integrated total approach of FM can more successfully bring improvement compared to regional unrelated treatments for people with multiple pain syndromes.
Alternative medicine? or new medicine?Is FM alternative medicine? No. The sense, control and coordination of movement are major preoccupations of the human brain. If musculoskeletal medicine includes muscle length and strength and joint range of motion then it can also include awareness of the sense, control and coordination of movement. This is not alternative medicine, it is medicine. FM is the art and practice of improving human function through awareness of the sense, control and coordination of movement. There is no comparable system yet developed or utilized in medicine. Physical Therapy & The Feldenkrais MethodFM is a stand alone process for movement education, posture and body-mind awareness. It can also be utilized in a rehabilitation setting as an adjunct to traditional medicine. Physical Therapy is ideally suited to adopting this methodology in its practice. |
| copyright © 1999-2004 robert j burgess. all rights reserved. |
3. UNIQUE REHABILITATION FEATURES OF THE FELDENKRAIS METHOD |
|||
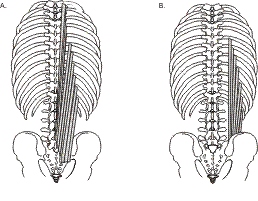
Motion parametersMotor control involves the sense and coordination between all body segments in internal and external space, the required forces to generate and control movement and the maintenance of balance during the performance of movement. Movement is thought to be controlled by combining synergies of a few basic motor primitives (Mussa-Ivaldi & Bizzi 2000). These are motion parameters of proprioception and also therefore of FM. FM involves hands on mobilizations and lessons in movement to improve awareness, sense and control of local and global motion parameters. Learning and treatmentSome chronic pains never go away. Sometimes people visit practitioners weekly for many years without any real true change to their chronic pain. In these circumstances clearly we don't yet have the answers and maybe also we are applying the wrong methodology. FM claims: “It can be healthier to learn than to be a patient or even be cured” The integration in FM of treatment with learning is a powerful tool. One major advantage of this methodology is that it is accumulative and not palliative. Back painTrunk anatomy defines trunk function. The largest muscles of the trunk span over the lumbar spine without attachment to it (Figure 1). These muscles originate on the pelvis and attach to the thorax especially the ribs. Longer muscles have greater strength and stability than smaller muscles (Crisco & Panjabi 1991). It makes sense to include both regional and global aspects of trunk function in the assessment of a person with low back pain. It has been determined that thoracic and pelvic limitations as well as diminished lumbar range of motion occur in subjects with chronic low back pain (Mayer 1984, Burgess et al 2003).
|
One major premise of FM is that poor motor control can lead to damage at points of increased stress and strain in the system: “Under ideal conditions the work done by the body passes lengthwise through the spine and the bones of the limbs, that is, in something as near to a straight line as possible. If the body forms angles to the main line of action, part of the effort made by the pelvic muscles will not reach the point at which it was directed; in addition, ligaments and joints will suffer damage....” (Feldenkrais 1972, p 89-90)
The Body-Mind PerspectiveThe application of FM to the rehabilitation setting provides a very gentle non invasive potent tool to improve human function. Dealing with tense motor habits associated with pain syndromes may reveal something of the self and emotions expressed in movement. On a deeper level the brain can only perceive the world (internal and external) through the senses including the proprioceptive sense. This can perhaps be defined as a third order of movement. As people progress with body and mind learning they become independent and self managing. |
| copyright © 1999-2004 robert j burgess. all rights reserved. |
4. FELDENKRAIS METHOD EXERCISES - Awareness Through Movement |
|||
|
|
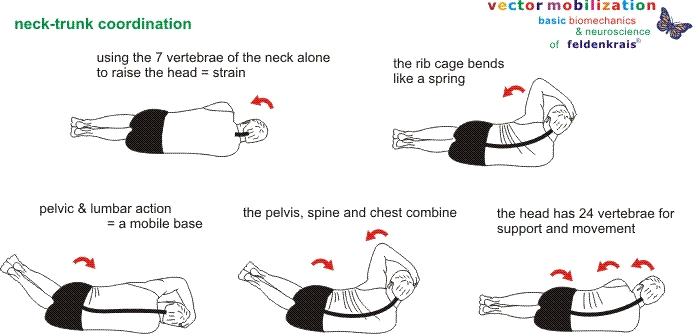
Head, Neck, Trunk and Pelvic Coordination
Above is an example of a movement process to discover the relationship between the head, neck and trunk. Using only the neck to raise the 10-12 pounds of the human head is a strain and is a primary contributor to neck pain. Learning to coordinate movement of the whole spine with the pelvis as the base makes for light work and no strain. This is optimization of CNS control of segment movement (Massion 1992). Notice that the thorax is illustrated as mobile and functioning as a “spring” like structure rather than a rigid “cage”. These exercises can be extended to a full 45 minute movement lesson or performed at home as shown above on this exercise sheet as part of a treatment program. This same methodology is apparent in all FM exercise classes and hands-on mobilization for motor control and awareness.
In a Nutshell
Next Issue: Managing Low Back Pain: A FM perspective. |
Figure 2. Leg-trunk coordination References1. Burgess, R. (2003). Trunk Kinematics. Doctoral Thesis Faculty of Health and Biomedical Sciences. Adelaide , University of South Australia 2. Crisco, J. J. d. and M. M. Panjabi (1991). The intersegmental and multisegmental muscles of the lumbar spine. A biomechanical model comparing lateral stabilizing potential. Spine 16 (7): 793-9. 3. Feldenkrais, M. (1972). Awareness Through Movement: Health exercises for personal growth. New York , Harper & Row Publishers. 4. Macintosh, J. E. and N. Bogduk (1987). The morphology of the lumbar erector spinae. 12 (7): 658-668. 5. Massion, J. (1992). Movement, posture and equilibrium: interaction and coordination. Prog Neurobiol 38 : 35-56. 6. Mayer, T., A. Tencer, et al. (1984). Use of noninvasive techniques for quantification of spinal range-of-motion in normal subjects and chronic low back dysfunction patients. Spine 9 (6): 588-595. 7. Mussa-Ivaldi, F. A. and E. Bizzi (200). Motor learning through the combination of primitives. Phil. Trans. R. Soc. Lond. B 355 : 1755-1769. |
| copyright © 1999-2004 robert j burgess. all rights reserved. |