2. Course Content
The Trunk as a Kinematic Chain from the Pelvis, to Thorax to Head and the Length of Spine. Local, adjacent, at a distance and global exercises and mobilizations drives a new motor control.
Pelvic Tilt. Which way do you tilt- anterior or posterior?
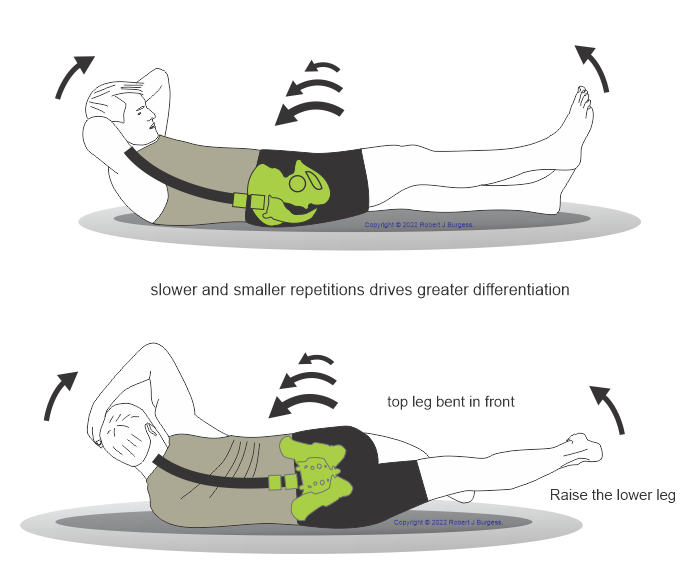
Leg-Trunk Coordination©, Arm-Trunk Coordination©- body segments working together.
The Hip Abduction Trilogy©. Empowering the Pelvis and Leg.
Body Segments or Muscles or Joints? Switching modes. What do Brains do?
Lumbo-Sacral Kyphosis: What we can learn from Isthmic Spondylolisthesis (IS) Research. IS sporned a major breakthrough in understanding sagittal alignment in all spinal conditions. It especially realised low lumbar kyphosis as a major factorin spinal disorders.
Pelvic floor- weak or over active? Strengthening or Skill Training and Stretching?
Passive Straight Leg Raise as a measure of Lumbar Mobility and Rigidity. The pelvis and lumbar spine are involved in PSLR.
Comparative vertebrate functional anatomy for understanding the human spine in action. For example: The Snake is all vertebrae and ribs just like our thorax. The thorax is designed to move. However, the Turtle's bony plates are also ribs!- evolution flattened the ribs. The turtle's spine is fused to the undersurface and obvisouly rigid. According to Gracovetski, we are lizards standing up on two legs.
Trunk Side Bending and Human Locomotion- spinal lengthening is a critical component of normal gait and human function. Old Dogs wag the tail alone on a rigid body. The Young Dog tails wags with the entire spine.
Immobility creates Instability. A review of literature on Spinal Instability. Does it exist?
The Kinematics of Lumbar DDD. Sagittal Alignment & Mobility of DDD. Natural History of the Spinal Sagittal Alignment.
Mobilizations for Motor Control©.
Lumbo-sacral mobilizations for flexion, side bend and traction motor control. Stretching the Pelvic Floor. |